Dr Ute Kruger Speaks About Vaccine-Induced Cancers
TRANSCRIPT
(0:07 - 0:21)
Welcome to this lecture. It is very nice to have you here. I have understood that you have a special background with what you have done.
(0:21 - 0:34)
You are a doctor at the regional hospital in Kalmar. You are also connected to the oncological department at the University Hospital in Lund, Sweden. You have been in Sweden for many years.
(0:35 - 0:57)
You were clinical supervisor and head of the pathological department at Växjö in Sweden. Before that, you did your doctorate and specialization in pathology at the University of Hamburg in Berlin. I understood that you did a very large study where you examined 8,000 patients.
(0:58 - 1:07)
You went through 8,000 patients from the large Berlin area. Not just one hospital, but many. You combined that with clinical diagnosis.
(1:07 - 1:22)
That is very exciting to do. It is through that that you became very interested in what is happening now around COVID-19. And clinical findings, especially with vaccine damage, which you will talk about now.
(1:23 - 1:32)
We look forward to hearing from you. Thank you very much for sharing this. Thank you.
(1:37 - 1:50)
Thank you for the invitation and thank you for the introduction. It is a shame that I did not have the opportunity to come to Oslo. I have worked in pathology for 25 years.
(1:50 - 2:10)
In the last 18 years, I have focused on breast cancer diagnosis. Here in the picture you can see my nice workplace in Kalmar. Seven years ago, I also had the opportunity to do research on breast cancer at Lund University.
(2:11 - 2:55)
Here I have examined 1,500 breast cancer cases in population-based patient material. Based on this background, I know roughly what the distribution should look like in terms of tumors and patient age, tumor size, malignancy, whether a tumor is better differentiated, i.e. grows slower, or whether it is poorly differentiated, i.e. grows faster and more aggressive. Almost a year ago, I got the feeling that I was getting samples from younger patients.
(2:55 - 3:12)
Here I mean patients born in the 70s or 80s. Even patients born in the 90s are now not uncommon among patients. These are patients who are in their 30s to 50s.
(3:15 - 3:31)
Then the tumors seem to be larger than usual. More than three centimeters large tumors are unusual in these times with mammography screening. But now I see a lot of large tumors.
(3:32 - 3:56)
Tumors in dimensions of more than four centimeters were previously rare, but are now relatively common. It is not uncommon to find tumors measuring 8 and 10 centimeters, even 12 centimeters. Two weeks ago, I saw a tumor that was 16 centimeters large, so the entire breast was covered with a tumor.
(3:59 - 4:22)
In addition, I rarely see multiple tumors, i.e. more than one tumor in the breast. Also bilateral, i.e. simultaneous tumor growth in both breasts, is sometimes seen. In contrast to the tumors themselves, I have a feeling that it grows more aggressively than before.
(4:26 - 4:43)
And since I love pictures, I would like to show some pictures for you. Here is a tumor that is well differentiated. When you do not know histology so well, you see that the light here is completely uninteresting.
(4:43 - 4:51)
It is fatty tissue. And then what is interesting is what is darker. It is the cartilages, it is the tumor as you can see here.
(4:53 - 5:07)
There is quite a lot of stroma between these tumor compounds. So that's what's a little brighter in the background. The tumor cells are relatively small and about the same size.
(5:10 - 5:22)
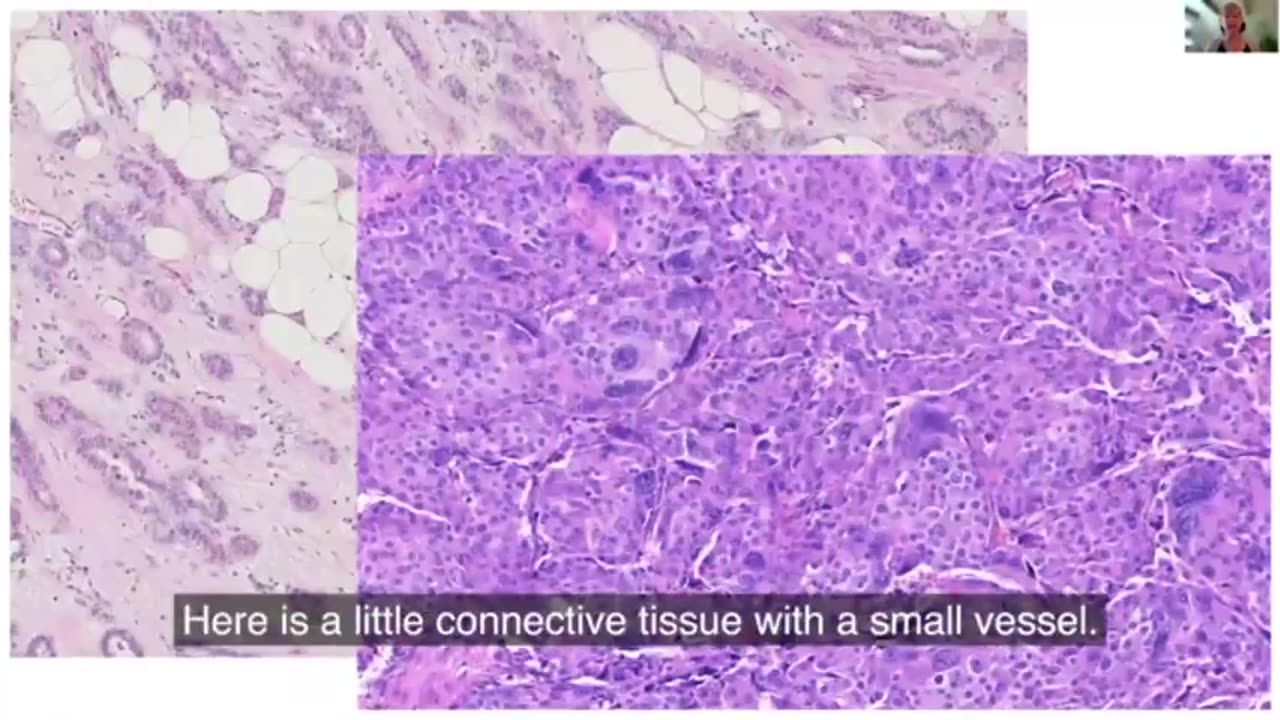
In the next picture, you see a poorly differentiated tumor, i.e. more aggressively growing. Here you hardly see any cartilage. There is a little cartilage here with a little core.
(5:23 - 5:42)
If you compare here on the first tumor, there is much more cartilage. Then there are very large, gigantic tumor cells with large cores. And if you compare, for example, this core with the one that is exactly next to it, it is also a tumor cell.
(5:42 - 5:59)
But there is a very large variation. In this picture, there are core division figures, i.e. everything that is marked with an arrow. It is mitosis, as you can see here.
(6:01 - 6:21)
It is the cells that are dividing. To visualize how many tumor cells are in division, there is a special coloration with antibodies. An immunohistochemical coloration called Ki-67.
(6:23 - 6:36)
Ki-67 is a proliferation marker. It is said that about two thirds of breast cancers are low proliferative. They grow slower.
(6:37 - 6:54)
A third are high proliferative, i.e. grow faster and more aggressively. If you look at an example, here is a Ki-67 coloration. You see a slightly different coloration than before in the routine coloration.
(6:56 - 7:09)
Then you see about the tumor we had before, with a lot of curls. As you can see here, now they are blue instead. You see these blue cores, they are negative.
(7:11 - 7:20)
Everything you see here. Then you see one strong brown core, and they are positive. They continue to proliferate.
(7:25 - 7:37)
You put the blue and brown cores in a relationship. Then you can enter a percentage. Here it is less than 10% when it comes to Ki-67.
(7:40 - 7:58)
If you look at a faster growing tumor, you see a much higher Ki-67 value. I do not see tumors that have such a Ki-67 value. It is almost 50% of the tumor cells that continue to proliferate.
(7:59 - 8:19)
Everything that is brown is positive, and everything that is blue is negative. This means that this tumor grows relatively fast. A few months ago, I thought that the patients did not want to go to the doctor due to the corona situation.
(8:21 - 8:34)
But it is over. There are more and more large and aggressively growing tumors in the material that I am examining. There is another change that I have discovered.
(8:36 - 8:59)
Lately, I have noticed that I have seen more patients who have had cancer for many years and are more or less temporarily declared. It can be cancer that patients have had, for example, 20 years ago. Relatively shortly after vaccination against Covid-19, the tumors explode and there is an extensive spread of cancer in the body.
(9:00 - 9:14)
The patients die a few months later. A current case that I have recently reported to the Medical Center is a woman in her 80s. She was operated on seven years ago.
(9:16 - 9:32)
A part of the breast with tumors had been removed earlier. Thereafter, there were no signs of tumors in the body. But now, three months after the third vaccine dose, she has felt a tumor that was rapidly growing.
(9:33 - 9:43)
It was measured in the operation preparation, 55 mm. At the same time, there were several skin metastases in the same breast. This is also very unusual.
(9:43 - 9:57)
You come with a residue and you already have metastases in the skin. Here is a picture of her current breast preparation. As you may remember, the light one is uninteresting, it is fat.
(9:57 - 10:06)
And then you see what is green marked here, the previous operating area. With a wind wave. There are hardly any cells here.
(10:07 - 10:24)
And then there is the red area. And this is the new cancer that is growing. It is of course much larger, but in this picture I thought it was nice to see that it was growing exactly into the previous breast area.
(10:26 - 10:48)
Another example was a woman in her seventies, who for many years had a metastatic, relatively slow-growing breast cancer. She lived with her metastases for three years. Among other things, there was a spread of telluric fluids, intestinal haemorrhage, skeleton and liver.
(10:50 - 11:22)
And shortly after vaccination against COVID-19, her tumor growth exploded in the liver. And the patient died within a few months. Even the clinic that had sent me a biopsy, i.e. a tumor cylinder of the liver, wrote on the prescription that it was unusual for the metastases in the liver to grow extremely fast, but that there was not as fast tumor growth in the other metastatic locations in the body.
(11:22 - 11:38)
In the microscope, I find parts of the tumor wall to the right. And in the middle here is her earlier cancer. This is a lobular cancer, a breast cancer.
(11:39 - 11:52)
And it grows diffusely infiltrating, or you can also see small rows of cells. And here in the middle you can see the tumor wall. It's like a lighter tumor wall, and the tumor cells are relatively small.
(11:53 - 12:27)
And to the left you can see the tumor that has occurred, an aggressively growing tumor, which is completely new in the liver. In the last three weeks, I have had three patient cases where there were several cancer diseases in different organs in the same patient a few months after the latest vaccination against COVID-19. These cancers had occurred in different organs at the same time.
(12:29 - 12:43)
This is also extremely unusual. One was, for example, a woman who got tests for her breast cancer. At the same time, lung cancer and pancreas cancer had been diagnosed.
(12:44 - 13:13)
This is very remarkable and unusual. All these cases that I suspect may be related to vaccination against COVID-19, I report to the Swedish Medicines Agency. And since there were a lot of reports, I was contacted by a clinical investigator at the Medical Insurance Unit at the Swedish Medicines Agency in November 2021.
(13:14 - 13:27)
He wondered how I was thinking and thought what I told was very interesting. So we booked a meeting where his boss would also be present. Of course, I was very happy and I felt heard.
(13:28 - 13:50)
But the next day, I just got a short email that there would be no meeting. And afterwards, I had another person who answered my questions on the Swedish Medicines Agency's website. Half a year ago, I attended a pathology conference in Germany.
(13:50 - 14:08)
There, I talked about my suspicions that vaccination against COVID-19 may be related to so-called turbo cancer. And I asked all the clinics for help to collect data to prove or contradict this hypothesis. Unfortunately, there was not much response.
(14:12 - 14:32)
In February this year, I did an interview with Miriam Reichel, who is a woman who herself has survived a cancer disease. She had received an eight-week prognosis from the doctor, but she defeated her cancer with, among other things, mental training and special treatment. This was 16 years ago.
(14:33 - 14:58)
Here I also learned that what we doctors learn at the university is apparently not the whole truth about diseases and healing processes in the body. But this was in parenthesis. There are now almost 223,000 clicks on this recording, and there are now 1,300 comments.
(14:59 - 15:36)
In these, you can read that there are many false descriptions and that there are more than me who believe that this vaccination may be related to rapid cancer development. Swedish researchers have already shown in vitro, i.e. in the reagent glass, that SARS-CoV-2 spike protein affects the DNA repair mechanism. I suspect that it is the same in vivo, i.e. in living organisms, and that this is why we see so many cancer diseases now.
(15:38 - 15:55)
All the pathologists I have spoken to are overloaded. There are now many more cancer trials than before. And now pathologists are mostly associated with oblivion, but that is only a very small part of the work of a pathologist.
(15:56 - 16:30)
I myself do not find myself oblivious much longer, but I have been oblivious several times lately. There are cases of death that I highly suspect are related to vaccination against COVID-19, and I would like to tell you about three such cases. One case involves a 60-year-old man who has had a malignant disease and who under ongoing cytostatic therapy has received a two-dose vaccine against COVID-19.
(16:30 - 16:57)
He developed relatively quickly symptoms of the so-called Guillauverie syndrome with alarm and died three months later. I found pronounced inflammation in the spinal cord and brain and inflammation in the skull, i.e. a vasculitis. Another case involves a woman in her 80s, who was alarmed a few months after vaccination.
(16:59 - 17:19)
I found a bleeding in the spinal cord in the neck area. I have blessed several hundred patients before, but I have never seen them like this before. In the microscope, I found in the area with the bleeding in the spinal cord, inflammation in the skull, i.e. the so-called vasculitis.
(17:20 - 17:34)
Clearly, the skull has burst due to the inflammation, and therefore there was bleeding. Small bleeds were also found in the brain. I also found inflammation in the heart muscle, i.e. myocarditis.
(17:36 - 18:00)
Then I would like to tell you about another case where the patient and the treating doctor suspected that the death could be related to the vaccination against COVID-19. But during the abduction, the pathologist could not find anything that indicated this. I have made the case a consultation, since the patient and the treating doctor did not believe in the abduction diagnosis.
(18:02 - 18:21)
So this is an earlier man in his 70s, who died after being vaccinated against COVID-19. Here I would like to show a histological average of the heart. Up here we have fat tissue again.
(18:22 - 18:32)
This is towards the outside of the heart. And what is a little pinkish, this is the heart muscle cell. As you can see, there are some different large cores.
(18:33 - 18:46)
The heart was also enlarged, so it was not healthy. But he had lived with it for many years before. And the problem here is that there are such bright areas as you can see.
(18:46 - 19:00)
Then there is a small area like this. And then here too. And this is Luka R, i.e. Luka R. So it is after an earlier injury where you see this.
(19:01 - 19:21)
And a regular pathologist should also see that there are far too many cells that lie between the heart muscle cells. So there is far too much going on in the background. And in the next picture you can see, when you look, you also find lymphoid infiltration.
(19:22 - 19:33)
Inflammatory cells are the dark dots, the lymphocytes. And they are here and they are not allowed to be here. They have nothing to do there.
(19:34 - 19:55)
So in summary, this is a picture of an older myocardial infarction, i.e. a heart muscle inflammation. And in the primary results of the doctor, there are no symptoms of myocarditis. I also see inflammation in the blood vessels, i.e. a vasculitis.
(19:55 - 20:04)
Here I have taken a picture from the lungs. And then you see here is the vascular wall. It is a venous vascular wall as you can see here.
(20:04 - 20:19)
And this is how it usually looks. But on that side, where there are rings, you can see that something is gnawing on the vascular wall from the inside. And then you see these dark dots again, i.e. the lymphocytes.
(20:20 - 20:42)
And then there are some inflamed cells, the macrophages, those that eat up the remains after inflammation. So this is a vascular wall with pronounced inflammation. And there were also bleeding in the lungs, partly fresh, partly older.
(20:42 - 21:03)
And this was clearly due to the fact that the vascular wall was damaged by the inflammation. In addition, I see a clear, fresh bump in a vascular wall in the heart. And I suspect that there are bumps in many of the venous organs.
(21:04 - 21:38)
However, special treatments are needed, which I cannot perform because I have only brought the glass to me. And since there is great discrepancy between my diagnosis and the original diagnosis of the doctor, I have consulted a pathologist colleague in Germany who has seen more than 20 cases of abduction where the patient had died after being vaccinated against COVID-19. He completely agreed with my assessment and that the death rate is highly suspected in connection with vaccination against COVID-19.
(21:41 - 22:01)
I see three major problems regarding abduction. The first is erroneous and missing data from the clinics, e.g. if the patient was vaccinated earlier or not. We have had several cases where the abduction report was wrong.
(22:01 - 22:23)
There is a field where it says the patient was vaccinated against COVID-19, yes, no. Or we have been told no, and if you look in the journal, you can see that the patient was certainly vaccinated. The other problem is that many of my pathologist colleagues do not participate in histological examinations, i.e. they do not perform a microscopic assessment.
(22:25 - 22:55)
For example, if you have a classic heart attack and you see a lump in a vein, then for many it is clearly a heart attack due to a thrombosis in the vein. But if you take histology, you can see that there is inflammation around the vein and that the inflammation actually causes the lump formation in the vein. So if you don't do histology, you miss it.
(22:57 - 23:20)
And the third problem is ignorance regarding the assessment of microscopic findings. In addition, I have a feeling that you don't want to see and interpret the changes in your context. Another problem is that, compared to me, hardly any other doctor in my area reports suspected cases to the Medicines Agency.
(23:23 - 23:49)
So, in summary, you work the vaccine against COVID-19 and, on the one hand, trigger fast-growing cancer or tubal cancer and, on the other hand, inflammatory conditions in the body, so-called autoimmune diseases. Cancer development may also be linked to the inflammatory conditions. I rarely see inflammatory changes in the cancer and in the surrounding vein.
(23:53 - 24:27)
And what I have described about cancer is clearly not just about breast cancer. I have heard from other pathologists who currently see an increased number of tumors that were previously hardly found, i.e. autoimmune tumors, and that the number of cancer cases over time has increased in the different organ areas. The changes I describe, which probably have to do with vaccination against COVID-19, are clearly just a fraction of what happens in the body.
(24:27 - 24:47)
I can say that I feel a little overwhelmed. I have studied medicine because I want to help people, but now it feels like I'm watching them die and I can't do much. You don't listen to what I say and my colleagues even question my competence.
(24:49 - 25:14)
I was consulted by a younger colleague about an abduction case and showed that there was a myocarditis and that the death could be linked to vaccination against COVID-19. My colleague didn't like that and he thought it was far too long-winded. And even if it wasn't my case, I registered it as a suspected case in the Medical Center.
(25:15 - 25:40)
I received very harsh criticism that I interfered in other people's cases and that I was even going to withdraw my application, which I refuse to do. More attentive doctors and researchers are needed who don't belong to this group as shown in this picture. Thank you for sharing your thoughts.
(25:46 - 25:58)
Yes, thank you very much, Ute. It was an incredibly exciting and important lecture. It will be published and seen by many here in Norway.
-
 15:59
15:59
ArynneWexler
8 hours agoAll The Reasons You're Right to Fear Zohran Mamdani | NN6
15.1K3 -
 LIVE
LIVE
Side Scrollers Podcast
12 hours ago🔴FIRST EVER RUMBLE SUB-A-THON🔴DAY 4🔴BLABS VS STREET FIGHTER!
1,283 watching -
 LIVE
LIVE
DLDAfterDark
4 hours ago $2.55 earnedGlock's Decision - How Could It Impact The Industry?
380 watching -
 25:57
25:57
The Kevin Trudeau Show Limitless
1 day agoThe Sound Of Control: This Is How They Program You
42.8K8 -
 8:29
8:29
Colion Noir
15 hours agoThree Masked Idiots Show Up at Her Door — Here’s What Happened Next
49.4K27 -
 15:38
15:38
Cash Jordan
9 hours agoPortland Zombies EMPTY 52 Stores… Mayor FREAKS as “Sanctuary” SELF DESTRUCTS
58.9K76 -
 1:23:21
1:23:21
Precision Rifle Network
1 day agoS5E4 Guns & Grub - Dustin Coleman of ColeTac
15K3 -
 1:09:25
1:09:25
Donald Trump Jr.
10 hours agoCorrupt UN Carbon Tax Exposed, Interview with John Konrad | TRIGGERED Ep.285
161K80 -
 42:58
42:58
TheCrucible
8 hours agoThe Extravaganza! EP: 59 with Guest Co-Host: Rob Noerr (10/23/25)
97.1K7 -
 1:40:59
1:40:59
Kim Iversen
9 hours agoTrump Threatens To End ALL Support For Israel
83.4K231