THE TOXIC TOOTH
A High-Level Guide to the Oral–Systemic Axis, Decision-Making, and Recovery
⸻
Survivor’s Testimony
“The Day My Mouth Finally Spoke”
I didn’t set out to become “the dental person.” I was a normal patient who trusted the system—right up until my body stopped cooperating.
1) Before the collapse
In 2006, my plan was simple: remove the metal from my mouth and be done with it. I booked with a local dentist, asked for non-metal restorations, and left believing we were on the same page.
We weren’t.
One of my largest cavities—originally filled with metal in childhood—was refilled with new metal after the old was drilled out. No discussion. No consent. I learned this only when I called about a strange metallic taste and the dentist said, breezily, “Yes, we went back in with amalgam—it’s durable.”
That tooth became a background character in my life—annoying, occasionally sensitive, easy to ignore. I moved on.
2) The slow drift into “mystery illness”
2011–2015 was a blur of airports and deadlines. I started grinding my teeth at night. Coffee tasted “hotter” on one side. I told doctors about heart flutters and static behind my eyes; they called it stress. By 2016, the symptoms stacked:
• Heart racing on stairs, then while sitting still
• Blood pressure spiking (the worst was 188/116 in urgent care)
• PVCs and PACs on a 48-hour Holter; “maybe early AFib” was mentioned, then retracted
• Head pressure, electric stabs behind the right eye, sound sensitivity
• Brain fog so thick I forgot simple words mid-sentence
• A hollow ache under my right cheekbone that nobody could localize
Cardiology found “nothing urgent.” Neurology said “migraine variant.” Primary care advised SSRIs. I tried to be grateful nothing “serious” was found, but I was falling apart.
The collapse arrived without warning. I blacked out at the kitchen sink, waking up in the open dishwasher amid forks and glasses. I remember being grateful I hadn’t impaled myself. Then the panic: my heart—wild, erratic, foreign.
3) The question no one had asked
Two days later, a friend asked, “Have you looked at your teeth?”
I’d told every specialist everything—except my dental history. It had never occurred to me. That night I ran my tongue along the back molars. The “refilled” tooth felt… thin. Cupped, almost. A crater I could catch with my tongue.
I booked with a dentist known for whole-health dentistry. The exam was different from anything I’d experienced: long history, bite analysis, thermal testing, percussion mapping, and a frank talk about materials. The X-ray showed a large, old restoration with recurrent decay; the tooth walls were paper-thin. A separate image flagged two root-canal teeth I’d half-forgotten from years earlier.
“Could this be connected to my heart stuff?” I asked, bracing for the eye roll.
“It can be,” the dentist said. “Not always. But sometimes the mouth is the missing chapter.”
For the first time in months, I felt seen.
4) The turning point—done safely, or not at all
We staged a plan: remove the failing restoration first and reassess—no heroics. On procedure day, the team worked with deliberate calm:
• Isolation and high-volume evacuation
• Copious water cooling and sectioning (not grinding)
• External air for me, air filtration in the room
• Slow, measured pace with breaks so my nervous system didn’t spike
Under the restoration, the tooth was practically a shell. The decay track ran under one cusp; the dentist showed me the photo: dark, undermined, fragile. We made the call—extraction instead of a last-chance crown that would likely fail.
I cried—not from pain, but from the relief of finally choosing.
We also scheduled the two root-canal teeth for separate days. “Staged” became my new religion. Before and after each appointment: hydration, minerals, protein, a binder my clinician recommended for me, and the most medicinal thing of all—sleep.
5) What changed (and how fast)
Day 1–3 after the first extraction:
The internal alarm quieted. Not silence—but lower volume. My resting heart rate dropped 8–10 bpm from my previous weeks. I felt a strange, clear emptiness where static had lived.
Week 2:
I slept through the night without that 3 a.m. cortisol bolt. The pressure behind my right eye eased. I could read for an hour without the words slipping away.
After the first root-canal extraction (week 4):
The stair-climb heart spikes stopped. Not “managed”—gone. My Holter later showed fewer ectopics. The second root-canal site was tougher—more swelling, a predictable dip week—but by week 8 the background dizziness that had made grocery stores a nightmare simply… wasn’t there.
Month 3:
If you’ve been ill a long time, you know the feeling: your body finally returns a “yes.” I wasn’t “cured.” I was responding—to sleep, to food, to sunlight. My capacity grew. That’s healing.
6) The moment that hardened my resolve
I asked for the extracted tooth “for the bag” and was told they couldn’t release it—too toxic to handle outside medical waste protocols.
So it was too toxic for a bag, but safe to sit 24/7 inches from my brain?
That contradiction snapped something in me. Not into anger—I’d wasted enough energy there—but into clarity. Whatever the debate on population-level risk, my body had just delivered its verdict.
7) What I did and didn’t do
• I did not rip everything out at once. Staging protected me.
• I did support “exits”: hydration, electrolytes, minerals, gentle walks, light sweating, bowel regularity.
• I did not chase random chelation threads online. I worked with a clinician who actually knew my labs and history.
• I did rebuild: protein at each meal, magnesium, trace minerals, time in the sun, a bedtime I respected like a prescription.
• I did get my bite and airway reassessed; less clenching meant less heat and stress on remaining teeth.
8) What the numbers and the mirror said
• Blood pressure stabilized from spikes (170–190 systolic at worst) to 120s/70s by month 3.
• Resting heart rate came down from the mid-80s to low 60s.
• My “brain fog meter” (a simple daily 1–10) moved from a stubborn 7–8 to a consistent 2–3 by month 4.
• HRV (on a consumer wearable—not perfect, but helpful) climbed steadily.
• Mostly: my face returned. The glassy stare faded. I recognized myself again.
9) What I wish someone had told me at the start
1. You’re not crazy—you might be contaminated. “Normal labs” do not negate lived reality.
2. Sequence over speed. The right next step beats an impressive plan.
3. Safety isn’t optional. Protective protocols aren’t “alternative”—they’re adult.
4. It may not be one thing. My keystones were a failing mega-restoration and two devitalized teeth; periodontal care and airway work kept the gains.
5. You will grieve. The years lost, the gaslighting, the money. Grieve—and move.
10) If you’re where I was
• Count what’s in your mouth. Write it down: how many metal restorations, which teeth are root-canaled, any extractions. Note when symptoms started or surged.
• Book with someone who respects both safety and symptoms. Ask about isolation, high-volume evacuation, coolant, room air, and staging.
• Don’t become a project. Become a person with a timeline: one step, then measure the response.
• Keep the nervous system in the loop. Breath, daylight, steady meals, gentle movement—your biology can’t heal if it thinks you’re sprinting from a fire.
11) Where I am now
I don’t tell this story to win an argument. I tell it because I got my life back—and because nobody asked me about my mouth until I was nearly unrecognizable to myself.
Today I work, walk, read, and laugh without budgeting every spoon of energy. I can sit with silence and feel calm instead of threat. Some days are still human. But the floor is higher, the spikes are rare, and my body feels like home again.
Was it the tooth?
It was the tooth plus process: a failing restoration removed carefully, devitalized teeth addressed thoughtfully, exits supported, bite and airway respected, time allowed.
Would I do it again?
Yesterday. With the same caution. With the same team. With the same refusal to rush.
If you’ve been living in a fog that no one can name, let this be permission to ask the unasked question:
What if the thing that broke me was already in my mouth—and what if removing it, safely and in sequence, is how I start coming back?
⸻
Plain-English note: This is one person’s experience, not medical or dental advice. If you’re considering changes, find qualified clinicians, insist on protective protocols, and move in stages you can recover from. Your body will tell you if you’re on the right road.
⸻
THE TOXIC TOOTH
A High-Level Guide to the Oral–Systemic Axis, Decision-Making, and Recovery
Prologue — A respectful wake-up
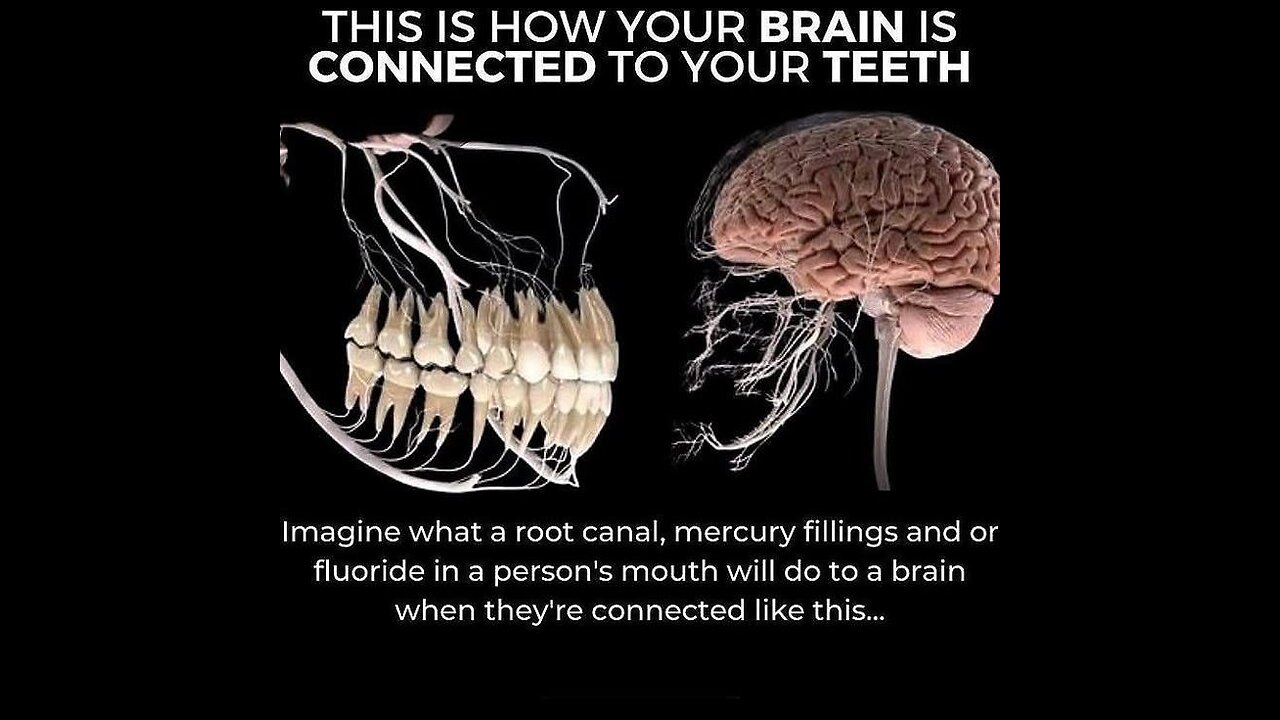
If your health story hasn’t added up—fatigue without labs, palpitations without cardiology answers, “brain fog” that isn’t just stress—the missing chapter may be the one medicine often skips: your mouth. This isn’t about fear. It’s about signal: local events in teeth, bone, and soft tissues can propagate through neural, immune, vascular, and endocrine networks. The aim of this paper is clarity, not controversy; prudence, not panic.
⸻
Part I — First principles (three things that are true at once)
1. The mouth and body are one system.
Nerves, microvasculature, lymphatics, and immune traffic make the oral cavity a high-leverage interface with the rest of you.
2. Materials and procedures matter.
Every restoration (metal or non-metal), every devitalized tooth, every extraction has properties (electrical, chemical, microbial) that can shape physiology.
3. Response is individual.
Exposure ≠ effect. Dose, genetics, nutrient status, stress load, sleep, infection, airway, and autonomic tone determine whether a given mouth becomes a non-issue or a bottleneck.
North Star: Replace ideology with informed consent, sequencing, and safety.
⸻
Part II — The Oral–Systemic Signal Model™
How local oral events can echo system-wide (four channels):
• Neural: Trigeminal and autonomic pathways modulate pain, muscle tone, heart rate variability, and stress response. Irritated dental or periodontal tissues can amplify sympathetic load.
• Immune: Chronic antigen stimulation (periodontal biofilm, necrotic dentin/bone) sustains cytokine signaling, raising systemic inflammatory tone and altering energy allocation (fatigue, malaise).
• Vascular/Microcirculatory: Toxins and inflammatory mediators alter endothelial function; microvascular sluggishness can feel like “low battery” cognitive and muscular output.
• Endocrine/Metabolic: Inflammatory and toxic stressors tug at thyroid/adrenal axes and insulin signaling; mitochondria—your energy factories—are exquisitely sensitive to redox imbalance.
Translation: “Symptoms” are often broadcasts from these channels, not random noise.
⸻
Part III — Situations worth a deliberate look
Not everyone has these. Not all are harmful. The point is evaluation quality, not blanket conclusions.
1) Legacy metal restorations (“silver” fillings)
• Typically include metallic mercury by design (as part of an amalgam alloy).
• Heat, chewing, and grinding can release small amounts of vapor; the practical impact varies by individual and burden.
• When attention is warranted: visible cracks/leakage; many large/old restorations; pregnancy/early childhood; kidney/neurologic vulnerabilities; symptom clusters that began or escalated after dental work.
2) Root-canal-treated teeth (devitalized, sealed)
• Many patients do well with them.
• Flags for second opinion: persistent ache/pressure, sinus tract, unusual sensitivity on percussion, repeated antibiotic courses, or a strong temporal link between placement and onset of systemic symptoms. Consider the tooth’s functional map (chewing load, airway impact) as well as standard imaging.
3) Post-extraction bone defects (poorly healed sites)
• After extractions (especially third molars), some individuals develop areas of low-grade necrosis or chronic infection that are easy to miss on basic imaging.
• When to explore: extraction history + stubborn vertigo, dysautonomia/POTS-like flares, facial/jaw oddities, or pain on palpation along the mandible/maxilla.
4) Galvanic interactions & mixed-metal mouths (advanced)
• Dissimilar metals can create microcurrents and local irritation. If symptoms are focal and conventional explanations fail, evaluating the electrochemical landscape may be appropriate.
5) Periodontal disease & airway (do not overlook the obvious)
• Chronic gum inflammation is a well-documented systemic stressor.
• Airway restrictions (tongue posture, nasal obstruction, sleep-disordered breathing) can magnify bruxism and clench-heat—worsening material wear and symptom load.
⸻
Part IV — Pattern recognition (not diagnosis)
May correlate in some patients; use as prompts for inquiry.
• Palpitations, episodic hypertension, “internal tremor”: devitalized upper molars/premolars or persistent periodontal inflammation → autonomic overdrive.
• Brain fog, light/noise sensitivity, “glass-behind-the-eyes” pressure: stacked restorations + nocturnal grinding → trigeminal stress + inflammatory load.
• Vertigo/imbalance, ear fullness, jaw clicking: poorly healed posterior mandible/maxilla post-extraction; TMJ/airway interplay.
• Crash-after-dental-work timeline: procedure → two to eight weeks of immune/metabolic wobble → partial recovery; repeats with each intervention when no protection/sequence is used.
Use these patterns to ask better questions, not to skip medical evaluation.
⸻
Part V — The Decision Frameworks
A) The Triage Ladder
1. Stability check: Is anything acutely infected, cracked, or failing? Fix that first.
2. Burden map: Count surfaces, note age/size of restorations, list root-canal teeth and extractions.
3. Symptom timeline: Mark any clear “before/after” inflection points around procedures.
4. Risk profile: Pregnancy plans, pediatrics, renal/neuro vulnerabilities, occupational exposures.
5. Readiness: Capacity for appointments, recovery, nutrition, sleep, stress support.
B) The S.A.F.E.R. Change Protocol™
• S—Sequence: Prioritize worst offenders; avoid “full-mouth marathons.”
• A—Avoid spikes: Protective measures during procedures to minimize exposure.
• F—Filtration & Field: Clean air, high-volume evacuation, coolant flow; manage electrical/mixed-metal issues thoughtfully.
• E—Exits & Enzymes: Support detox routes (bowel/urine/sweat/lymph) and tissue turnover with clinician-guided nutrition and binders where appropriate.
• R—Rebuild & Regulate: Minerals, protein, mitochondrial cofactors, autonomic downshifting (breath, sunlight, gait).
C) The 80/20 Evaluation
• 20% of findings create 80% of relief. Start where risk × plausibility is highest (e.g., a symptomatic devitalized tooth, a fractured large restoration), reassess after each step.
⸻
Part VI — Implementation: How to do this without making it worse
1) The team (and what to ask)
• Dentist (restorative/biological): “What isolation and evacuation do you use? How do you cool and section restorations? What’s your step-down plan?”
• Endodontist/Oral surgeon: “What’s the decision logic for retreat vs extraction? How do you confirm resolution?”
• Physician/integrative clinician: “How do we coordinate pre-/post-procedure labs and recovery support?”
• Hygienist: “What’s the personalized periodontal plan while we work upstream?”
2) Protective essentials (principles)
• Barrier isolation, high-volume evacuation, copious water cooling, clean room air, appropriate patient/staff respiratory protection.
• Gentle sectioning rather than aggressive bulk grinding.
• Clear plan for staging (weeks between sessions) and post-care.
3) Three sequencing scenarios
• Conservative: Address one failing restoration or one suspicious tooth → reassess symptom trajectory → proceed.
• Standard: Replace a quadrant of aging restorations with protection; address one high-suspicion devitalized tooth; re-image old extraction site if symptomatic.
• Advanced: Staged full-mouth revision over months with comprehensive recovery protocols and physician coordination.
⸻
Part VII — Recovery physics (what improvement tends to feel like)
Weeks 1–2: Less “internal static,” steadier pulse, sleep normalizes; mild swings are common.
Weeks 3–8: Baseline clarity returns; inflammation feels lower; exercise tolerance and mood rise together.
Months 3–6: Energy reliability improves; fewer post-stress dips; cognitive endurance rebuilds.
Months 6–12: Structural stability (bite, airway, posture) + metabolic steadiness consolidate gains.
Trajectories differ; the signal to watch is capacity, not perfection.
⸻
Part VIII — Myth / Reality Matrix
• Myth: “If I have metal fillings, I’m doomed.”
Reality: Many people tolerate them; others don’t. The state of the restoration, your risk profile, and procedure safety matter more than ideology.
• Myth: “Root canals always cause disease.”
Reality: Many patients do fine. Some don’t. Persistent symptoms around a specific tooth merit skilled evaluation, not automatic extraction.
• Myth: “Detox will fix everything.”
Reality: Reducing exposure without safe process can make things worse. Sequence + support first; then rebuild.
• Myth: “If imaging is clean, I’m fine.”
Reality: Some problems are functional or micro-architectural; combine imaging with exam, history, and response to staged interventions.
⸻
Part IX — Tools you can use this week
The 7-Minute Mouth Audit
• Count metal restorations; note age/size.
• List devitalized teeth and extraction sites.
• Mark any tooth that feels “not part of me.”
• Draw a symptom timeline with dental events.
• Choose one concrete question for your next visit.
Scripts (copy/paste)
To a dentist:
“Before we plan anything, can we review materials, integrity, and options? If we replace, what protective steps do you use? How would you sequence my case to minimize stress and exposure?”
To a physician:
“I’m pursuing a staged oral evaluation. Can we coordinate on sleep, stress, basic labs, and post-procedure support so I don’t crash the system while we make changes?”
Your Personal Research Log (one page)
• Today’s energy: □ low □ medium □ high
• Sleep quality: □ poor □ ok □ solid
• Triggers noticed: ________
• Mouth sensations (ache/pressure/temperature): ________
• Next step scheduled: ________
⸻
Part X — Ethics, consent, environment
• Informed choice: Know what’s in your mouth, what can replace it, and the tradeoffs.
• Do-no-harm sequencing: Smaller, safer steps beat heroic marathons.
• Environmental stewardship: Materials and removal choices should protect you, staff, and the environment.
⸻
Part XI — Research priorities (where intelligent readers can help)
1. Better characterization of individual susceptibility (genetics, redox/mitochondrial status).
2. Standardized diagnostics for post-extraction bone defects.
3. Prospective studies on autonomic metrics (HRV) before/after staged dental interventions.
4. Pragmatic trials comparing protective protocols and patient-reported outcomes.
5. Integrated oral–systemic care pathways (dentistry + medicine) with cost/benefit analyses.
⸻
Closing — Replace certainty theater with intelligent action
You don’t need to pick a side. You need a process: Observe, prioritize, protect, stage, support, and measure. For some, the mouth is background. For others, it’s the keystone. Either way, the route out is the same: clarity over panic, safety over speed, function over dogma.
You’re not broken. You may be overloaded.
That’s not a verdict—it’s a map.
⸻
Plain-English disclaimer
This document is educational, not individualized medical or dental advice. Decisions about replacing restorations, addressing devitalized teeth, or exploring bone surgery should be made with qualified clinicians who can evaluate your specific case and coordinate care.
-
 4:36
4:36
FragmentsOfTruth
7 days ago🜏 The Forbidden Current — Tesla’s Lost Blueprint for Limitless Power
378 -
 1:03:23
1:03:23
Tactical Advisor
13 hours agoNew Gun Unboxing | Vault Room Live Stream 044
235K39 -
 19:12
19:12
Robbi On The Record
14 hours ago $19.02 earnedThe Loneliness Epidemic: AN INVESTIGATION
70.4K94 -
 14:45
14:45
Mrgunsngear
1 day ago $113.27 earnedFletcher Rifle Works Texas Flood 30 Caliber 3D Printed Titanium Suppressor Test & Review
121K29 -
 17:17
17:17
Lady Decade
1 day ago $8.18 earnedMortal Kombat Legacy Kollection is Causing Outrage
79.7K14 -
 35:51
35:51
Athlete & Artist Show
1 day ago $14.15 earnedIs Ryan Smith The Best Owner In The NHL?
92.5K11 -
 22:56
22:56
American Thought Leaders
2 days agoCharles Murray: I Thought Religion Was Irrelevant to Me. I Was Wrong.
75.8K39 -
 36:22
36:22
Brad Owen Poker
15 hours agoGIGANTIC $17,000+ Pot In BOBBY’S ROOM! TRAPPING Top Pro w/FULL HOUSE!! Big Win! Poker Vlog Ep 326
80K8 -
 3:53
3:53
GreenMan Studio
1 day agoRUMBLE RUNDOWN: DREAM HACK SPECIAL W/Greenman Reports
64.6K13 -
 1:28
1:28
Damon Imani
2 days agoThey Laughed at Trump’s Cognitive Test — Damon Made Them REGRET It!
61.7K40