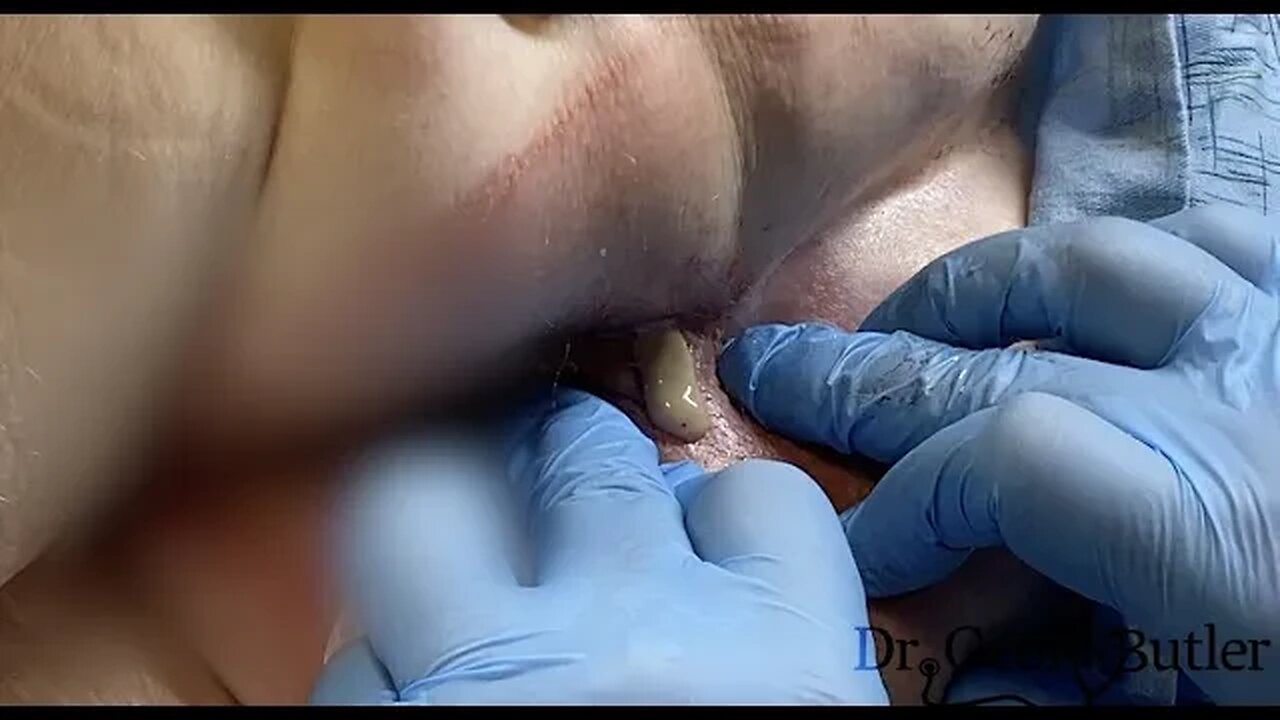
Drainage of an Ischiorectal Abscess (READ CAPTION)
WARNING - GRAPHIC CONTENT (READ CAPTION)
First, I would like to thank this patient for allowing us to video tape this case as this is clearly a very sensitive area and this procedure is quite painful. As a result it is hard to demonstrate these cases and consequently students and residents get very little exposure to them. HOWEVER, if these are not drained, the patient can become critically ill and some very nasty complications can develop.
Second, like most infected fields, but for this one in particular, many of you, including those in the medical field might comment on how poor the anesthesia is and how barbaric it may be to move ahead when the patient is uncomfortable. HOWEVER, you cannot do a circumferential block here because of the nature of the anatomy. As well, switching to a general anesthetic is not something most general surgeons will do as that conveys risks, in and of itself to the patient, and access to OR suites can be limiting as well. Furthermore, the ischiorectal space can be massive, and as you'll see, the amount of infection will typically render local anesthetic almost useless.
Finally, as to the procedure itself, you have a lot of bad options open to you. You want to avoid the rectum itself as you can lacerate the sphincter and that is a disaster. Furthermore, you don't want to make a massive incision as the anaesthesia is very poor and to do so would be cruel to the patient. As a result, will there be some retained infection? Yes, there will be. HOWEVER, this will drain if you pack it and create an opening that will allow the infection to egress. During this procedure you will appreciate that the entire right ishiorectal space is infected, spanning an area of about 10-15 cms. As well, you'll see during the procedure that an area opens just above the rectum obviously secondary to a communication with the central cavity. Again, you should not be extending any type of opening here as the complications can be significant.
As a last note, I have seen this patient in follow up and he is healing well but slowly. He is on 2 antibiotics and I did not reinsert any packing after the first day. The lower 2/3 of this space has cleared very nicely but the upper third, while improving, is doing so much slower, which isn't unexpected.
I imagine I will catch a lot of negative comments for this video, which is fine. If you have legitimate questions or concerns I will make an effort to answer them.
For those who celebrate, Happy Easter and please be respectful to the patient. Take care.
-
 LIVE
LIVE
Forrest Galante
9 minutes ago6 Deadliest Man Eaters to Ever Exist
1,081 watching -
 10:14
10:14
MattMorseTV
5 hours ago $3.71 earnedThe EU is in HOT WATER.
26.5K21 -
 LIVE
LIVE
Mally_Mouse
5 hours agoSpicy Saturday!! - 10k CELEBRATION! - Let's Play: Labyrinthine
485 watching -
 37:09
37:09
The Mel K Show
6 hours agoMel K & Dr. Kirk Moore | A Doctor’s Oath: Doing What is Right No Matter the Cost | 7-26-25
14.4K5 -
 36:44
36:44
NordicVentures
5 days ago $0.71 earnedWINTER Bushcraft 2 Nights: Building ALONE a Survival Shelter
6.52K4 -
 LIVE
LIVE
JakRazGaming
3 hours ago $0.09 earnedPlaying Minecraft with GameQuest1552, Rexmon, and JuicyKinnKandy! Stream 9
59 watching -
 LIVE
LIVE
GoA_Malgus
2 hours agoGoA Malgus - The Legend Has Returned!!! - Live domination on Black Ops 6
51 watching -
 7:12
7:12
nospeedlimitgermany
2 days ago $0.97 earnedAudi TT 1.8 T Roadster | 180 PS | Top Speed Drive German Autobahn No Speed Limit POV
9.93K1 -
 LIVE
LIVE
CharleyHornsePlays
1 hour agoCHP DESTINY 2 | Big noob | WEEKLY DONOR GIVEAWAYS
54 watching -
 4:15:37
4:15:37
FrizzleMcDizzle
4 hours ago"She Who Plays with Wonder" AXON BOSS?! - Clair Obscure: Expedition 33
2.71K